 Official Site of The State of New Jersey
Official Site of The State of New Jersey
New Jersey Medicaid Continues to Fund Poor Quality Care for Nursing Home Residents
- Posted on - 03/31/2023
Table of Contents
Executive Summary
This report provides a current list of the 12 New Jersey nursing homes that have consistently received the lowest-possible quality rating but continue to be paid tens of millions of dollars in Medicaid funds. [1] This report is the second follow-up to an Office of the State Comptroller (OSC) report first issued just over a year ago, in February 2022. In that report, OSC made similar findings—15 nursing homes in New Jersey’s Medicaid program performed poorly year after year without facing any consequences.[2]
The nursing homes’ poor performance has real and potentially fatal consequences for residents. State inspectors have found widespread and harmful conditions at the lowest-rated facilities. In some, residents face conditions that include abusive staff members, clogged toilets, broken doors and furniture, poorly maintained and dirty facilities and patient rooms, understaffed shifts, and untrained staff administering medications. And for some of these facilities, these sorts of issues have existed in various forms for nearly a decade.
In OSC’s first report on this topic, OSC made several recommendations. The goal of these recommendations was to move New Jersey’s Medicaid program away from a system that continues to pay significant amounts for consistently poor-quality nursing homes and replace it with one that rewards nursing homes that obtain higher ratings and provide higher-quality care. OSC made these recommendations to the New Jersey Department of Human Services, Division of Medical Assistance and Health Services (DMAHS), which oversees Medicaid providers, and the New Jersey Department of Health (DOH), which oversees nursing homes.
OSC recommended that DMAHS institute a phased approach to tie quality of care to admissions, including curtailing and/or capping admissions to nursing homes that consistently perform poorly, and in some cases, removing existing Medicaid beneficiaries from nursing homes that fail to improve. OSC further recommended that DMAHS eliminate or reduce the amount of the quality incentive program payments (QIPP) made to these poor-performing nursing homes. OSC also recommended that DMAHS and DOH collaborate to bar owners of the consistently lowest-performing nursing homes from obtaining interests in, or contracts with, additional nursing homes. Many of the owners of the nursing homes on OSC’s list owned or operated other nursing homes, some of which were also consistently poor performers.
With one exception, DMAHS has disregarded OSC’s recommendations. DMAHS followed OSC’s recommendation to stop paying QIPPs to the lowest-performing nursing homes.[3] Otherwise, DMAHS has elected to continue the policies criticized in OSC’s reports. Under longstanding flexibility afforded by federal law to states, DMAHS could have adjusted its policies to implement OSC’s recommendations. This flexibility was recently endorsed by the White House and the Centers for Medicare & Medicaid Services (CMS), which encouraged states to be more assertive in protecting residents of nursing homes.
In response to OSC’s recommendations, DMAHS notes that “the state’s approach to improving quality has leaned towards defining standards and providing support for all facilities to meet them.” It contends that it is “required to respect the autonomy of individuals and families as they select where and how to access Medicaid benefits.” DMAHS declines to use its Medicaid funding power to incentivize high-quality care and to dis-incentivize consistently low-quality care, writing that “[a]lthough some facilities may be low performers, they remain licensed by CMS and DOH to provide these services.” [4]By accepting the status quo and continuing to pay for poor quality, DMAHS fails to recognize that even if it decreased funding for facilities with low-quality care, individuals and families would still have the autonomy to select other higher-quality facilities.
DOH, for its part, contends that it has taken multiple steps to improve quality of care in nursing homes through inspections and penalties, and has shared this data with DMAHS and the public. DOH also claims that it considers the track record of owners in issuing a new license or transfer of ownership.
Nevertheless, OSC’s latest review demonstrates that, thus far, the approaches taken by DMAHS and DOH are not working—the consistently lowest-rated nursing homes are still providing poor-quality care; most of the facilities targeted for improvement through the Special Focus Facility (SFF) program have not improved; and several of the owners of these lowest-rated facilities continue to own or operate multiple nursing homes.
Specifically, this report finds the following:
- Seven of the twelve lowest-rated nursing homes identified in this report were also identified in OSC’s original report, issued over a year ago;
- Only one of the twelve nursing homes identified in this report has shown any signs of recent improvement;
- Using OSC’s methodology, three facilities showed no improvement at all over the review period;
- Several of the facilities on OSC’s list have provided sub-standard care for nearly a decade;
- In the past three years, three of the four “graduates” of the SFF Program, a program designed to improve nursing home quality, have reverted to one-star ratings; and
- Twenty owners/operators/administrators of one of the lowest-rated facilities own multiple nursing homes in New Jersey, with four owning or operating multiple facilities on OSC’s lowest-rated list.
OSC’s overall findings here are almost identical to the original report—the consistently lowest-rated nursing homes continue to provide poor-quality care while continuing to be financed with public funds. As this report is issued, over a year after OSC first sounded the alarm, more than 1,500 Medicaid beneficiaries continue to receive care in these persistently lowest-rated nursing homes—facilities that have been consistently cited for serious failings in patient care, medical management, nutritional services, and overall environment.[5] And New Jersey continues to pay an average of more than $102 million a year for this poor-quality service.[6]
Background
OSC is an independent agency responsible for monitoring and auditing government programs and agencies; reviewing the efficiency and effectiveness of government functions and programs; identifying cost savings, preventing misconduct within the programs and operations of government agencies; and investigating fraud, waste, and abuse. OSC is charged with implementing the Medicaid Program Integrity and Protection Act, N.J.S.A. 30:4D-53 to -64, by, among other things, ensuring that the State spends its Medicaid resources in a responsible and effective manner. OSC performs these duties through its Medicaid Fraud Division.
A. New Jersey Medicaid
Medicaid is a joint federal and state program administered by states. The New Jersey Department of Human Services, Division of Medical Assistance and Health Services (DMAHS) administers the Medicaid program and provides health insurance for approximately 2.2 million residents, including residents who are aged, blind, disabled, and those with low- and moderate-income.[7] In state fiscal year (SFY) 2023, the Legislature budgeted more than $17.96 billion in state and federal funds for New Jersey’s Medicaid program.[8] In 2022, New Jersey’s Medicaid program paid $1.72 billion to nursing homes.[9]
B. DOH Authority to Regulate and Inspect Nursing Homes
The New Jersey Department of Health (DOH) serves as the state regulatory agency for nursing homes. It licenses and oversees the enforcement of regulations for nursing homes in New Jersey. DOH employees inspect nursing homes on behalf of the Centers for Medicare & Medicaid Services (CMS). DOH reports its findings to CMS, which incorporates these findings into its rating assessment tool to determine nursing home ratings. Both DOH and CMS maintain reports of the federal inspections on their websites. Separately, DOH has its own statutory authority to license and inspect nursing homes, approve changes of ownership, investigate potential noncompliance, demand corrective/remedial actions, curtail admissions, impose penalties, and take other enforcement steps.[10]
Through the health-inspection process, DOH inspectors determine whether there are deficiencies; establish each deficiency’s impact on residents (severity); and ascertain how many residents are affected (scope). A facility is given a score that ranges from “A” to “L.” A scope and severity score of “L” is the most serious finding because it means that there was widespread harm and “immediate jeopardy.” In contrast, a scope and severity score of “A” is the least serious finding because it means that there was an isolated incident with no actual harm and little potential for harm. According to DOH, immediate jeopardy describes “a situation in which immediate corrective action is necessary because the facility’s noncompliance with one or more requirements of participation has caused, or is likely to cause, serious injury, harm, impairment, or death to a resident receiving care in a facility.”[11]
DOH inspectors survey New Jersey’s nursing homes and provide their findings to CMS. The data that results from those inspections allows CMS to compare the quality of nursing homes over multiple years, using a one- to five-star rating system, with one star being the lowest and five stars being the highest. CMS compiles this information in its Care Compare website.[12]
C. CMS's Five-Star Rating System
CMS’s five-star rating system uses information from health inspections (both standard and complaint-based), certain defined quality measures, and staffing levels to develop a score for each facility. The health inspection score is, however, the linchpin of the rating system.[13] This score is developed based on unannounced site visits, conducted by a team of state inspectors from DOH, who spend several days in the nursing home assessing a variety of practices and policies in such areas as resident rights, quality of life, medication management, skin care, resident assessment, nursing home administration, environment, and kitchen/food services. After CMS establishes a nursing home’s health inspection score, it adds or subtracts points based on the nursing home’s quality and staffing measure scores to arrive at an aggregated score. For a nursing home to be among the lowest performers for the first month of each quarter for at least six of the past eight quarters, it means that the nursing home consistently has had more widespread, serious, and uncorrected deficiencies than nursing homes with higher star ratings. According to CMS, “nursing homes with 1 star are considered to have quality much below average.”[14]
Methodology
OSC examined CMS Care Compare data from 2013 to 2023, focusing on data from April 2021 to January 2023, to assess whether New Jersey nursing homes that accept Medicaid beneficiaries performed poorly over an extended number of years.[15] Through this review, OSC identified 12 nursing homes that received one-star ratings for the first month of six of the past eight quarters (i.e., January, April, July and October). This methodology is consistent with the approach OSC used in its two prior reports on this topic. Throughout this report, OSC refers to these 12 one-star nursing homes as the “12 lowest-rated nursing homes.”
During this review, OSC also analyzed publicly available inspection reports for the facilities on the list, as well as ownership information and other relevant data.
Prior to issuing this report, OSC contacted DMAHS and DOH to request that each provide an update on the actions it took to implement the recommendations contained in OSC’s February 2022 report. OSC also provided each agency with a draft of this report for comment and updated this report, as appropriate, based on their responses.
Findings
A. New Jersey's lowest-rated nursing homes have consistently performed poorly for many years.
In Table A below, OSC identifies the 12 nursing homes that received one-star ratings for the first month of six of the past eight quarters. In other words, during the two years of OSC’s review period, on eight reporting periods, these nursing homes received one-star ratings at least 75 percent of the time. These facilities have been consistently cited for deficiencies in patient care, medical management, nutritional services, and overall environment.
Table A: 12 Lowest-Rated Nursing Homes[16]
Facilities listed in RED were included on OSC’s Lowest-Rated LTC List in February 2022 and September 2022.
|
Name |
Location |
NJ Medicaid Payments (SFY 2017- 2022)[17] |
|
|
CEDAR GROVE RESPIRATORY AND NURSING CENTER1 |
Williamstown, NJ County: Gloucester |
$62,449,497 |
|
|
DEPTFORD CENTER FOR REHABILITATION AND HEALTHCARE* |
Deptford, NJ County: Gloucester |
$75,657,458 |
|
|
FOREST MANOR HCC |
Hope, NJ County: Warren |
$21,801,519 |
|
|
GROVE PARK HEALTHCARE AND REHABILITATION CENTER†2 |
East Orange, NJ County: Essex |
$49,388,907 |
|
|
HAMILTON GROVE HEALTHCARE AND REHABILITATION, LLC~* |
Hamilton, NJ County: Mercer |
$48,655,603 |
|
|
PALACE REHABILITATION AND CARE CENTER |
Maple Shade, NJ County: Burlington |
$60,680,487 |
|
|
PHOENIX CENTER FOR REHABILITATION AND PEDIATRICS~3 |
Haskell, NJ County: Passaic |
$81,308,450 |
|
|
PREMIER CADBURY OF CHERRY HILL*4 |
Cherry Hill, NJ 08002 County: Camden |
$20,735,737 |
|
|
SILVER HEALTHCARE CENTER*5 |
Cherry Hill, NJ County: Camden |
$85,105,316 |
|
|
SOUTH JERSEY EXTENDED CARE* |
Bridgeton, NJ County: Cumberland |
$41,111,349 |
|
|
STERLING MANOR |
Maple Shade, NJ County: Burlington |
$37,795,130 |
|
|
WARREN HAVEN REHAB AND NURSING CENTER~6 |
Oxford, NJ County: Warren |
$29,836,562 |
|
|
* Identified by the CMS Special Focus Facility Program in January 2023, due to its history of serious quality issues. † Identified by CMS as being cited for abuse. ~ Included on OSC’s Lowest-Rated LTC List in September 2022. |
|||
|
1. formerly Meadowview Nursing and Respiratory Care – 2019 2. formerly New Grove Manor – 2021 3. formerly Wanaque Center for Nursing and Rehabilitation – 2019; Wanaque Convalescent Center – 2014 4. formerly Cadbury Nursing and Rehabilitation Center – 2016 5. formerly Alaris Health at Cherry Hill – 2016; 6. formerly Warren Haven – 2015 |
|||
[1] Cedar Grove Respiratory and Nursing Center and Silver Healthcare Center are skilled nursing facilities and/or ventilation units that receive higher per patient reimbursement rates.
[1] Cedar Grove Respiratory and Nursing Center and Silver Healthcare Center are skilled nursing facilities and/or ventilation units that receive higher per patient reimbursement rates.
Table B reveals that these 12 lowest-rated nursing homes include three that received one-star or less for all eight quarterly intervals in the review period—South Jersey Extended Care, Sterling Manor, and Warren Haven Rehab and Nursing Center. In other words, using OSC’s methodology, these facilities showed no improvement over the entire review period. These three facilities collectively earned $108 million from SFY 2017 to 2022 for these sub-par services.[18]
For six more facilities, the results were only marginally better—they began with one-star ratings, briefly rose to two-star ratings for just one or two rating periods, and then returned to a one-star rating for the remainder of the period. Only one facility ended the two-year review period with a better star-rating than it had at the beginning of the period.
Table B: Ratings of 12 Lowest-Rated Nursing Homes: April 2021 to January 2023
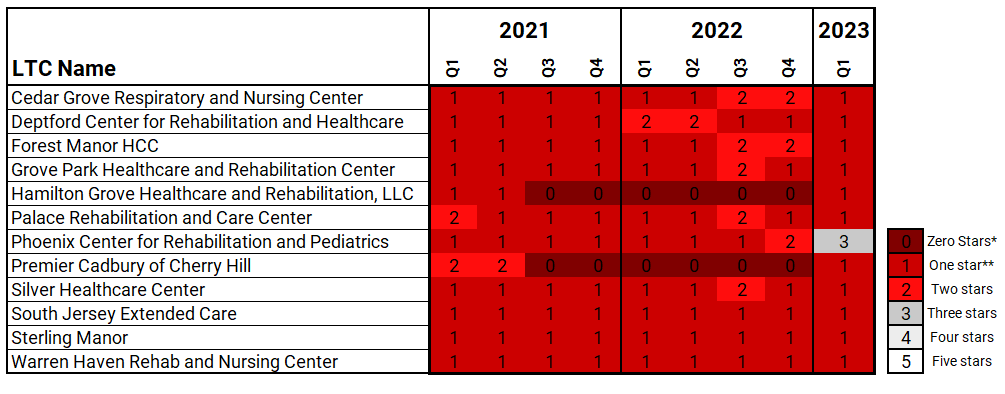
*Facilities with a zero rating are low rated and in a CMS Special Focus Facility Program.
**One star is the lowest-possible rating. Five stars is the highest.
The 12 lowest-rated facilities collectively received about $614 million in Medicaid funds over the last five years. This means that, on average, the New Jersey Medicaid program collectively paid these facilities more than $102 million per year.
Table C demonstrates that several of the 12 nursing homes have been among the lowest-rated nursing homes going back at least to 2013. Others appear to have deteriorated over the past few years and remained low. Some experienced rapid declines and have remained among the lowest-rated in recent years. In sum, these 12 nursing homes currently provide low-quality care to their residents, and many of them have been providing low-quality care for an extended period of time, in some cases for nearly ten years.
Table C: New Jersey’s Lowest-Rated LTCs Fail to Improve Over Time
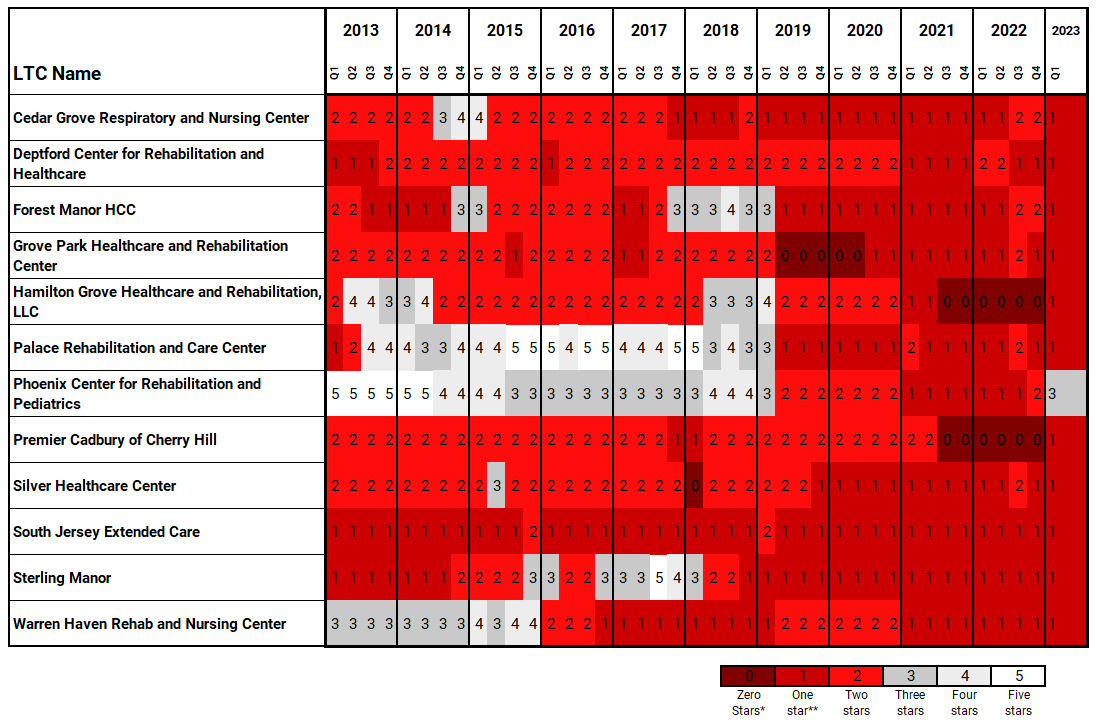
*Facilities with a zero rating are low rated and in a CMS Special Focus Facility Program.
**One star is the lowest-possible rating. Five stars is the highest.
The duration of these poor ratings is deeply troubling. New Jersey has discretion to refuse to pay for chronically poor-quality care and yet persists in doing so. History has shown that, in the absence of some meaningful consequence, many of the lowest-rated nursing homes will not improve. Unless the state meaningfully changes its approach to overseeing and funding these facilities, it will continue to spend hundreds of millions of dollars of taxpayer funds on the lowest-rated nursing homes, and Medicaid beneficiaries will continue to suffer the often terrible, frequently dangerous, and sometimes fatal consequences.
B. Inspections revealed significant deficiencies at the lowest-rated facilities -- putting residents' health and safety at risk.
OSC reviewed recent health inspection reports of the 12 lowest-rated nursing homes and found persistent deficiencies. These deficiencies are notably not all of the deficiencies that are present in each of these nursing homes; they are only the deficiencies that were observed while the inspectors were in the building for a period of days.
According to the reports compiled by DOH inspectors, daily life at these facilities is filled with all sorts of indignities, from chronically cold meals to excrement-stained rooms. Some of the facilities are worse than others, but they are all deficient in ways that indicate they provide substandard care. At Silver Healthcare Center, a DOH inspector found that residents at risk for aspiration were not provided with the appropriate liquids to prevent asphyxiation, which could result in choking or even death. At Grove Park Health Care and Rehabilitation Center, a DOH inspector found three times over a period of six days, that a resident’s fingernails were overgrown and jagged, with a “black substance” visible under the nails.
Residents’ personalized care plans, created by physicians, were often disregarded. At Phoenix Center for Rehabilitation and Pediatrics, the report found that residents were given incorrect feeding tube formulas. At Hamilton Grove Healthcare and Rehabilitation, DOH inspectors found that feeding tubes were improperly administered, creating a risk of aspiration pneumonia, a lung infection that can be fatal. An inspector reported that two residents at Forest Manor HHC had visible bruises on their faces; one of them had fallen repeatedly at the nurses’ station, and the inspector said the facility’s documentation showed no action was identified to prevent future falls.
In a few cases, DOH found alleged abuse of residents, which the facility had not documented or reported to authorities, as required. According to DOH, a South Jersey Extended Care resident was “roughly handled” by two employees, causing the resident to fall out of the wheelchair onto the floor; the resident landed in the hospital with chest pain. At Silver Healthcare Center, DOH reported that one patient had an unexplained broken arm, and the incident was never investigated.
The examples above are just a few of the deficiencies noted in DOH’s inspection reports.[19] While the average DOH inspection results in a finding of five deficiencies, some of these facilities had as many as 30 deficiencies noted in a single report. Some deficiencies included widespread incidents of immediate jeopardy to residents’ health and safety.
Table D shows the date of the most recent CMS routine inspection, a link to the report, the number of deficiencies per facility, and highest scope and severity level for each of the 12 lowest-rated nursing homes.[20] As noted in OSC’s February 2022 report, high scope and severity deficiency findings are far more likely in a nursing home with a one-star rating than a nursing home with a five-star rating.[21]
Table D: 12 Lowest-Rated Nursing Homes -- Most Recent Routine Inspections
|
Name |
Most Recent Inspection |
Number of Deficiencies |
Highest Scope & Severity Level [22] |
|
CEDAR GROVE RESPIRATORY AND NURSING CENTER |
02/23/2022 |
17 |
F- Widespread; Severity Level 2; No actual harm, potential for more than minimal harm |
|
DEPTFORD CENTER FOR REHABILITATION AND HEALTHCARE |
09/20/2022 |
23 |
F- Widespread; Severity Level 2; No actual harm, potential for more than minimal harm |
|
FOREST MANOR HCC |
08/24/2021 |
2 |
G – Isolated; Severity Level 3; Actual harm that is not immediate jeopardy |
|
GROVE PARK HEALTHCARE AND REHABILITATION CENTER |
02/18/2022 |
12 |
L – Widespread; Severity Level 4; Immediate jeopardy to resident health or safety |
|
HAMILTON GROVE HEALTHCARE AND REHABILITATION, LLC |
5/20/2022 |
2 |
L – Widespread; Severity Level 4; Immediate jeopardy to resident health or safety |
|
PALACE REHABILITATION AND CARE CENTER, THE |
03/31/2022 |
18 |
F- Widespread; Severity Level 2; No actual harm, potential for more than minimal harm |
|
PHOENIX CENTER FOR REHABILITATION AND PEDIATRICS |
8/31/2022 |
10 |
L – Widespread; Severity Level 4; Immediate jeopardy to resident health or safety |
|
PREMIER CADBURY OF CHERRY HILL |
10/18/2022 |
3 |
K – Pattern; Severity Level 4; Immediate jeopardy to resident health or safety |
|
SILVER HEALTHCARE CENTER |
08/29/2022 |
30 |
L – Widespread; Severity Level 4; Immediate jeopardy to resident health or safety |
|
SOUTH JERSEY EXTENDED CARE |
12/30/2021 |
7 |
K – Pattern; Severity Level 4; Immediate jeopardy to resident health or safety |
|
STERLING MANOR |
02/23/2022 |
21 |
J – Isolated; Severity Level 4; Immediate jeopardy to resident health or safety |
|
WARREN HAVEN REHAB AND NURSING CENTER |
7/18/2022 |
7 |
K – Pattern; Severity Level 4; Immediate jeopardy to resident health or safety |
C. New Jersey's nursing homes failed to improve under CMS's Special Focus Facility Program.
CMS established the Special Focus Facility (SFF) Program to help states identify and improve quality of care in nursing homes with a history of serious quality issues, systemic problems, and repeated offenses.[23] Through this program, CMS identifies a list of potential candidates in each state based on weighted results of the last three standard inspections and complaint inspections from the past three years.
For New Jersey, CMS provides DOH with a list of ten candidate facilities each month from which DOH selects facilities to participate, with a maximum of two facilities remaining in the program at a time. For each SFF-selected facility, DOH then must perform a full onsite inspection every six months and use progressive enforcement until the facility graduates from the SFF program or is terminated from Medicaid. After a facility graduates or is terminated, DOH selects a new SFF from the monthly list.
As explained by CMS, graduation from SFF does not mean there are no longer quality issues in the facility; however, there should be an “upward trend in quality improvement.” CMS monitors graduates for three years post-graduation. DOH previously reported that there have been no facility terminations as a result of the SFF program. DOH recently selected Silver Healthcare Center, one of the facilities on OSC’s current lowest-rated nursing home list, to participate in the SFF program.[24]
As shown in Table E below, three of the four nursing homes that “graduated” from the SFF program within the past three years remain on the lowest-rated nursing home list, and one, Premier Cadbury of Cherry Hill, is again an SFF program candidate after just graduating in 2022. The failure of these nursing homes to improve their performance indicates that the SFF program is not working as intended. Despite pouring state resources into assisting these facilities, the SFF program failed to improve the quality of these nursing homes.
Table E: SFF Graduates 2020-2023
|
Facility Name |
Date of Graduation |
Months as an SFF |
Currently on OSC’s Lowest-Rated List? |
Current Overall Rating |
|
Grove Park Healthcare and Rehabilitation Center |
03/23/2020 |
24 |
Yes |
1 |
|
Hamilton Grove Healthcare And Rehabilitation, LLC |
08/04/2022 |
16 |
Yes |
1 |
|
Premier Cadbury Of Cherry Hill |
11/15/2022 |
19 |
Yes |
1 |
|
Cornell Hall Care and Rehabilitation Center |
12/07/2020 |
19 |
No |
3 |
Shortly after OSC published its February 2022 Report, the White House issued a statement titled “Protecting Seniors by Improving Safety and Quality of Care in the Nation’s Nursing Homes,” in which it announced reforms intended to ensure “poorly performing nursing homes are held accountable for improper and unsafe care and immediately improve their services or are cut off from taxpayer dollars.”[25] This statement included plans to improve the quality of care in nursing homes and hold poor-performing facilities more accountable by raising minimum staffing requirements, increasing scrutiny of poor performance under the SFF Program, expanding penalties and sanctions, and increasing ownership/financial transparency.
In follow-up to the White House’s press release, CMS issued an October 2022 Memorandum to state survey agency directors (including DOH), in which CMS acknowledged that SFF graduates at times failed to improve and outlined revisions to improve the SFF program.[26] CMS announced that it was establishing a more stringent set of progressive enforcement tools, including requirements that state survey agencies impose penalties immediately upon issuing a finding, increased penalties for ongoing deficiencies, higher penalty limits, and an admission prohibition for any nursing home that failed to comply with prior agency findings.
D. Numerous owners of the lowest-rated nursing homes have interests in other nursing homes in New Jersey.
OSC’s February 2022 report highlighted that owners of some of the lowest-performing nursing homes also own/manage/administer other nursing homes. That trend continues with the current list. Twenty of the owners/managers/administrators of the 12 lowest-performing nursing homes own multiple nursing homes in New Jersey. The four individuals listed below own or manage multiple facilities on OSC’s 12 lowest-rated nursing home list. One of these individuals is affiliated with 43 nursing homes in New Jersey. Set forth below is a breakdown of the affiliations of all four of these owners, managers, and administrators, as of January 2023.[27]
- Zev Farkas owns:
- Forest Manor (since 2012), which has maintained an overall rating of one since April 2019, with the exception of two quarters, in which it scored an overall rating of two; and
- Warren Haven (since 2015) which has maintained an overall rating of one or two since first quarter 2016.
- Marc Weisz is affiliated with three nursing homes and Steven Krausman is affiliated with four nursing homes in NJ. Marc Weisz owns and Steven Krausman manages:
- South Jersey Extended Care (since 2002), which has maintained an overall rating of one for the last ten years, with the exception of two quarters, in which it scored an overall rating of two; and
- Sterling Manor (since 2002), which has maintained an overall rating of one every quarter since the fourth quarter of 2018.
- Sam Stern is affiliated with a total of 43 nursing homes in NJ, 18 of which received an overall rating of two or lower in January 2023. He is an officer of:
- Palace Rehabilitation (since 2007), which has maintained an overall rating of one since April 2019, with the exception of two quarters, in which it scored an overall rating of two; and
- Silver Health Care Center (since 2017), which has maintained an overall rating of two or lower for the last ten years, with the exception of one quarter in which it scored an overall rating of three in 2015.
Attached as Exhibit A is a chart showing more comprehensive ownership information for the 12 lowest-rated nursing homes, including the roles and percentages, if available.[28]
E. DMAHS's response to OSC's February 2022 recommendations and OSC's reply.
OSC’s February 2022 report urged DMAHS to adopt a phased approach to connect nursing home quality of care to Medicaid beneficiary admissions and Medicaid payments. It also recommended that DMAHS modify the Medicaid Quality Incentive Payment Program (QIPP) to cease paying nearly identical incentive amounts to the lowest-rated nursing homes as it did the highest performers. The goal was to end the status quo of allowing a substantial number of Medicaid beneficiaries to receive care in persistently low-performing nursing homes that received large amounts of public funds. OSC recognized that implementing policies to achieve this goal may require DMAHS to adopt regulations, request CMS to approve state plan amendments, or take other steps to obtain federal approval.
OSC asked DMAHS to provide details regarding steps it had taken to implement the recommendations in OSC’s February 2022 report. In response, DMAHS pointed to efforts by DOH, including DOH’s data dashboard, which was required by legislation.[29] DMAHS also noted its collaboration with DOH to address Woodland Behavioral and Nursing Center (Woodland), describing how “[i]n an unprecedented action, DOH and Human Services jointly moved for the appointment of a receiver to manage and eventually close the troubled facility.” DMAHS also explained that it continued to “evaluate long-term strategies for nursing facility quality improvement.” Finally, DMAHS advised that it had modified QIPP eligibility to exclude nursing homes that received a one-star overall rating, nursing homes that were a CMS Special Focus Facility, and/or nursing homes that had two or more high-severity deficiencies during a DOH inspection. These changes effectively excluded each of the 12 lowest-rated nursing homes from the QIPP in SFY 2023.
DMAHS’s response did not directly address OSC’s core recommendation–that DMAHS implement a phased approach to connect quality of care to receipt of Medicaid funding, which, in successive steps, may include imposing programmatic sanctions, such as issuing an order barring further Medicaid admissions, capping the total number of Medicaid beneficiaries, and/or, if necessary, removing existing Medicaid beneficiaries. DMAHS suggested it would not implement OSC’s recommendation because of “limitations of the CMS Star Rating system.” DMAHS stated that its approach to improving nursing home quality has focused on “defining standards and providing support for all facilities to meet them.” DMAHS also noted that it is focused on protecting individual choice by nursing home residents, stating that it is “required to respect the autonomy of individuals and families as they select where and how to access Medicaid benefits.” Finally, DMAHS pointed out that “[a]lthough some facilities may be low performers, they remain licensed by CMS and DOH to provide these services.”
DMAHS’s policy decisions elevate certain goals and interests over others. Allowing residents to choose to receive poor-quality care does protect individual choice but comes at the cost of exposing vulnerable New Jerseyans to harm in nursing homes that are perpetually the lowest-rated. This approach also fails to take into account that denying access to low-performing nursing homes would still leave individuals and families with the autonomy to select higher-quality nursing homes. DMAHS’s choice to fund poor-quality facilities as long as they remain licensed by DOH demonstrates that DMAHS is not willing to exercise its independent authority to decide which nursing homes will and will not receive Medicaid beneficiaries and funding.
Instead, under DMAHS’s approach, unless and until nursing homes are ordered closed by CMS or DOH, which DMAHS admits was, until recently, an “unprecedented action,” these lowest-rated nursing homes will continue to house Medicaid beneficiaries and be paid with public funds for doing so. DMAHS has pointed OSC to its role in the closure of Woodland—an action that was initiated by CMS in 2022 after over two years of troubling reports and a long history of poor ratings going back to 2013.[30] But in doing so, DMAHS fails to recognize that, using OSC’s methodology, a few of the facilities on OSC’s current list rival Woodland when it comes to the duration of poor-quality care.
In making these decisions, DMAHS has not only rejected OSC’s core recommendation but also declined an invitation from the federal government to be creative in addressing the issue of low-quality nursing home care. CMS recently encouraged states to use existing flexibility to establish Medicaid payment rates that promote better quality of care and health outcomes in nursing homes. Also, in an August 2022 bulletin, CMS reminded state Medicaid programs, including New Jersey, that they have the ability to implement initiatives through the Medicaid state plan, waiver, or demonstration processes. CMS explained that states have “broad flexibility to design their provider payment structures.”[31] Finally, CMS challenged state Medicaid programs to use data and stakeholder feedback to “inform innovative payment policies that help strengthen safety and quality of care in nursing facilities.”
These directives echo OSC’s recommendation to DMAHS to connect nursing home quality of care to admissions and Medicaid payments. In declining to use the power granted to it by federal law, despite CMS’s encouragement to do so, DMAHS is electing to maintain the status quo and tolerating ongoing and seemingly perpetual poor performance in the lowest-rated nursing homes identified in this report.
F. DOH's response to OSC's February 2022 recommendations and OSC's reply.
OSC’s February 2022 report urged DOH to collaborate with DMAHS in implementing a phased approach to block owners of the lowest-performing nursing homes from owning interests in other nursing homes in order to link quality of care to state licensure and Medicaid payments. Likewise, OSC recommended that DOH obtain guidance from the Long-Term Care Ombudsman (LTCO) on approaches to nursing home quality of care issues.
In response to OSC’s inquiries, DOH noted that it carefully follows state and federal guidelines with respect to surveys and inspections. When appropriate, it penalizes nursing homes, curtails admissions, and in rare cases, issues termination of payment notices. DOH stated that it makes inspection and other information available to DMAHS and the public. DOH cited its role in the response to the conditions at Woodland and a COVID-19 outbreak at another facility. DOH also stated that it currently conducts track record reviews for changes or transfers in ownership in accordance with applicable regulations. DOH also criticized OSC’s reliance on the CMS star-rating, advising that it has developed a better indicator of poor performance than CMS’s star-rating system. DOH contended that OSC’s approach would dis-incentivize the purchase of the nursing home by new owners who may improve the facility and may result in facilities closing and in residents being displaced. DOH emphasized that its goal is to remediate facilities and keep residents in their homes.
These efforts, which have not been evaluated by OSC because they are outside the scope of this review may, in time, result in improvements to nursing home quality. But, based on the data, it does not appear that they have resulted in noticeable change since OSC’s February 2022 report. The fact remains that, as with Woodland, many of the nursing homes in this report have been low performers for nearly a decade and have shown little or no recent improvement. Seven of the twelve nursing homes on OSC’s current list were also listed in OSC’s February 2022 report. Three of the four facilities that graduated from the SFF program are currently rated as one-star facilities. While DOH’s efforts may, in the future, improve quality, history shows that without a significant change, many of the lowest-rated facilities will continue to provide poor-quality care.
Recommendations
OSC offers the following updated recommendations to improve the quality of care for Medicaid beneficiaries in nursing homes and to prevent waste of Medicaid funds:
- As recommended in OSC’s February 2022 Report, DMAHS should establish a phased approach to compel the lowest-performing nursing homes to improve their quality of care. This may include issuing an order barring further Medicaid admissions, capping the total number of Medicaid beneficiaries, encouraging and arranging for voluntary moves of existing residents, and other measures to protect Medicaid beneficiaries. The phased approach should be based on the star-rating system used by CMS or some other system that identifies perpetually poor-performing nursing homes.
- DOH should bar owners/managers/administrators of any of the lowest-performing nursing homes from obtaining interests in additional nursing homes and, in collaboration with DMAHS, from receiving Medicaid funds, until such time as the lowest-performing nursing home(s) is no longer listed among the lowest performing nursing homes.
[1] Nursing homes are also known as long-term care facilities, LTCs, or LTCFS. This report will primarily use the term “nursing home” throughout.
[2] The nursing homes addressed in this report are long-term care facilities (nursing homes) licensed by DOH. This report does not include the following DOH-licensed facilities: residential health care facilities, assisted living residences, comprehensive personal care homes, adult day cares, assisted living programs, adult family care, pediatric day cares, or dementia care homes.
[3] See Division of Aging Services FY2023 Nursing Home Rates https://www.state.nj.us/humanservices/
doas/documents/Copy%20of%20Fiscal%20Year%202023%20NH%20Rates%20for%20FFS%20Residents%20_NF%20QIPP-%2012122022.xlsx, last accessed March 28, 2023.
[4] See Exhibit A.
[5] OSC accessed CMS Care Compare data on the number of residents per day for each nursing home on the lowest-rated nursing home list, in order to determine an approximate number of Medicaid beneficiaries.
[6] OSC downloaded NJ Medicaid payment data from fiscal years 2017, 2018, 2019, 2020, 2021 and 2022 from the NJ Medicaid System/Shared Data Warehouse and combined Medicaid claims payment data for both Fee for Service and Managed Care Organizations for total payment amounts. The amounts provided are estimates/averages and do not account for future claim edits and/or retractions.
[7] See NJ FamilyCare Total Enrollment: https://njfamilycare.dhs.state.nj.us/analytics/home.html, last accessed March 28, 2023.
[8] See NJ Legislature Analysis of DHS Budget, State Fiscal Year 2022-2023: https://pub.njleg.state.nj.us/
publications/budget/governors-budget/2023/DHS_analysis_2023.pdf, last accessed March 28, 2023.
[9] OSC downloaded NJ Medicaid payment data from fiscal years 2017, 2018, 2019, 2020, 2021 and 2022 from the NJ Medicaid System/Shared Data Warehouse and combined Medicaid claims payment data for both Fee for Service and Managed Care Organizations for total payment amounts. The amounts provided are estimates/averages and do not account for future claim edits and/or retractions.
[10] See DOH website: https://www.nj.gov/health/healthfacilities/, last accessed March 28, 2023.
[11] See DOH Scope and Severity Definitions: https://healthapps.state.nj.us/facilities/fsss.htm, last accessed March 28, 2023.
[12] See CMS Care Compare website: https://www.medicare.gov/care-compare/?providerType=Nursing
Home, last accessed March 28, 2023.
[13] See CMS Nursing Home, Care Compare Technical Details: https://data.cms.gov/provider-data/topics/ nursing-homes/technical-details, last accessed March 28, 2023.
[14] CMS Five-Star Quality Rating System: https://www.cms.gov/medicare/provider-enrollment-and-certification/certificationandcomplianc/fsqrs, last accessed March 28, 2023.
[15] See CMS Nursing Home Data Archive: https://data.cms.gov/provider-data/archived-data/nursing-homes, last accessed March 28, 2023.
[16] OSC excluded Sycamore Living at East Hanover because there is not enough data to calculate the rating.
[17] Cedar Grove Respiratory and Nursing Center and Silver Healthcare Center are skilled nursing facilities and/or ventilation units that receive higher per patient reimbursement rates.
[18] OSC downloaded NJ Medicaid payment data from fiscal years 2017, 2018, 2019, 2020, 2021 and 2022 from the NJ Medicaid System/Shared Data Warehouse and combined Medicaid claims payment data for both Fee for Service and Managed Care Organizations for total payment amounts. The amounts provided are estimates/averages and do not account for future claim edits and/or retractions.
[19] Information obtained from each facility’s CMS Care Compare Page, as of March 27, 2023.
[20] Information obtained from each facility’s CMS Care Compare Page, as of March 27, 2023.
[21] See Abt Associates, Nursing Home Compare Five-Star Quality Rating System: Year Five Report, Figures 3.1b and 3.1c, June 16, 2014: https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/
CertificationandComplianc/Downloads/NHC-Year-Five-Report.pdf, last accessed March 28, 2023.
[22] Information obtained from each facility’s NJ DOH page, as of January 31, 2023.
[23] See GAO website: https://www.gao.gov/products/gao-10-197#:~:text=The%20Centers%20for%20Medi
care%20%26%20Medicaid,address%20poor%20nursing%20home%20performance, last accessed March 28, 2023.
[24] See CMS SFF List: https://www.cms.gov/medicare/provider-enrollment-and-certification/certification
andcomplianc/downloads/sfflist.pdf, as of January 25, 2023.
[25] See White House press release: https://www.whitehouse.gov/briefing-room/statements-releases/2022/
02/28/fact-sheet-protecting-seniors-and-people-with-disabilities-by-improving-safety-and-quality-of-care-in-the-nations-nursing-homes/, last accessed March 28, 2023.
[26] See CMS Memorandum: https://www.cms.gov/files/document/qso-23-01-nh.pdf, last accessed March 28, 2023.
[27] See CMS Nursing Home Data Archive, Ownership Table: https://data.cms.gov/provider-data/archived-data/nursing-homes, last accessed March 28, 2023.
[28] This chart is based on data available through the CMS Provider Enrollment, Chain, and Ownership System (PECOS).
[29] See P.L.2021, c.457: https://pub.njleg.state.nj.us/Bills/2020/PL21/457_.PDF and NJ DOH Nursing Home Facility Data website: https://www.nj.gov/health/ltc/nursing-homes/, last accessed March 28, 2023.
[30] See CMS LEGAL PUBLIC NOTICE of DISCRETIONARY TERMINATION FROM MEDICARE/MEDIAID [sic] PROGRAM: https://www.cms.gov/files/document/new-jersey-woodland-behavioral-and-nursing-center-05
-26-2022.pdf, last accessed March 28, 2023.
[31] See CMS Bulletin, Medicaid nursing facility payment approaches to advance health equity and improve health outcomes. – August 22, 2022: https://www.medicaid.gov/federal-policy-guidance/downloads/
cib08222022.pdf, last accessed March 28, 2023.

Waste or Abuse
Report Fraud
Waste or Abuse
