 Official Site of The State of New Jersey
Official Site of The State of New Jersey
Sources
{kind=link}
General questions
The “Reopening Directive” for long-term care facilities refers to Executive Directive NO. 20-026 which initially signed by Health Commissioner Judith Persichilli on August 10, 2020 and was most recently revised on October 20, 2020.
Recognizing the impact that COVID-19 has had a long-term care facilities across the State, this Directive calls for a phased in reopening of nursing homes and sets a number of requirements relating to infection control (e.g., minimum infection control programs and staff), response readiness (e.g., staffing, PPE), and allowed activities for each phase.
The Directive’s phased approach to reopening long-term facilities is largely dependent on New Jersey’s progression through the statewide stages of recovery (i.e., Road Back to Recovery)
Phase 0: Any facility with an active outbreak of COVID-19, as defined by the Communicable Disease Service (CDS), per the COVID-19 Communicable Disease Manual Chapter, any facility that cannot attest to criteria to advance phases, and all facilities if New Jersey is in maximum restrictions per the Road Back to Recovery: https://covid19.nj.gov/faqs/nj-information/reopening-guidance/when-and-how-is-newjersey-lifting-restrictions-what-does-a-responsible-and-strategic-restart-of-new-jerseyseconomy-look-like
Phase 1: Facility that has never had an outbreak or that concluded an outbreak, and 14 days have passed since New Jersey moved to Stage 1 (May 2, 2020) of the Road Back to Recovery and the facility has submitted all the attestations required in this Directive (described below)
Phase 2: Facility that has never had an outbreak or that concluded an outbreak, and 14 days have passed since New Jersey moved to Stage 2 (June 15, 2020) of the Road Back to Recovery and the facility has submitted all the attestations required in this Directive (described below)
Phase 3: Facility that has never had an outbreak or that concluded an outbreak, and 14 days have passed since New Jersey moved to Stage 3 (DATE TBD) of the Road Back to Recovery and the facility has submitted all the attestations required in this Directive (described below)
As New Jersey is currently in Stage 2 and 14 days have passed since the day it moved to Stage 2, any facility that has concluded an outbreak and submitted all required attestations will move to Phase 2 (i.e., will proceed from Phase 0 to Phase 2 and skip Phase 1).
14 days after New Jersey moves to Stage 3, any facility that has concluded an outbreak and submitted all required attestations will move to Phase 3 (i.e., will proceed from Phase 0 to Phase 3 and skip Phases 1 and 2).
The definitions of “active outbreak” and “concluded outbreak” are detailed below.
Information about current reopening phase of each LTC Facility can be found here
To move beyond Phase 0, each LTC Facility must have concluded its outbreak (if it had one previously) and submit 8 attestations that covers areas such as creation of an “outbreak plan” (covering communications, staffing, testing, data reporting), use of infection control precautions (including hiring of dedicated staff, stockpiling of PPE, visitations restrictions), development of a respiratory protection program for staff, agreement to participate in national data reporting, and reporting of current outbreak status.
The full list of attestations and the requirements to fulfill each attestation are summarized below:
Appendix: Key attestations in Reopening Directive
- Phased reopening attestation which requires
- “Outbreak plan” including communication methods to notify patients/residents, their families or guardians and staff about any infectious disease outbreaks and includes strategies and methods for virtual communications in the case of visitation restrictions, at a minimum on a weekly basis
- Not experiencing a staffing shortage and has a documented plan for securing additional staff
- CMS-certified facilities must have a documented communication plan and must inform residents/families by 5 p.m. the next calendar day following the subsequent occurrence of either: each time a single confirmed infection of COVID-19 is identified, or whenever three or more residents or staff with new-onset of respiratory symptoms occur within 72 hours of each other
- Displaying prominently on websites and social media a method for communicating complaints or urgent calls
- Meeting testing and data reporting requirements set by the State
- Infection control contract
- If facility has more than 100 beds or has on-site hemodialysis services, it must have entered a contract for infection control services
- If facility has less than 100 beds or no on-site hemodialysis services, it must have entered a contract for infection control services based on the resident population and facility service needs identified in the facility risk assessment
- Infection control employee
- If facility has more than 100 beds or has on-site hemodialysis services, it must have hired a full-time infection control employee by August 10, 2021.
- If facility has less than 100 beds or no on-site hemodialysis services, it must have staffed the Infection Prevention and Control (IPC) program based on the resident population and facility service needs identified in the facility risk assessment
- Respiratory protection program implementation
- Facility must have implemented a respiratory protection program that complies with the OSHA respiratory protection standard for employees.
- PPE stockpile
- If facility is standalone or not part of a system with 8+ facilities, it must have 2 months of PPE on hand
- If facility is part of a system with 8+ facilities, it must have at least 1 month of PPE on hand
- Facilities should use the CDC’s PPE Burn Rate Calculator in order to estimate the amount of PPE needed (https://www.cdc.gov/coronavirus/2019-ncov/downloads/hcp/PPE-Burn-RateCalculator.xlsx).
- National Health Safety Network – Data reporting
- Facilities must have registered, authorized NJDOH to access data, and enter information in the NHSN COVID-19 Module a minimum of twice weekly
- End of outbreak (or no outbreak experienced)
- Facilities must attest date they their outbreak(s) have concluded or attest that they have never experienced an outbreak
- Phase II indoor visitation attestation
- Facilities must have a mechanism to collect informed consent from the residents and visitors, a location designated for indoor visitation, sufficient staff, and a mechanism for appointments and sufficient PPE to permit visitation.
Once the above criteria are met, the Phase to which the LTC Facility progress is dependent on the State’s current stage of reopening. As New Jersey is currently in Stage 2 and 14 days have passed since the day it moved to Stage 2, any facility that has concluded an outbreak and submitted all required attestations will move to Phase 2 (i.e., will proceed from Phase 0 to Phase 2 and skip Phase 1).
Note that the detection of a new COVID-19 outbreak returns the facility to Phase 0 regardless of the facility’s current Phase.
Facilities must comply with certain infection control requirements in order to advance phases and must complete the following:
- Facilities must use the CDC’s burn rate calculator and they must calculate their stock at the burn rate of the surge of COVID 19 in their facilities or at the peak of residents in their facility.
- Facilities that belong to a system with 8 or more facilities must have 1 month of PPE in stock.
- Facilities that are not part of a system, must have 2 months of PPE in stock. This is for emergency use only and not daily use.
- Facilities must enter into a contract for infection control services or they must hire a full-time employee if they have more than 100 beds or hemodialysis;
- Facilities with ventilator beds are required to hire an infection control employee in accordance with current statute;
- Must have an outbreak plan that includes lesson learned from COVID 19 and must include a communication plan in the event of visitation restrictions due to an outbreak or emergency;
- Facilities must post the outbreak plan publicly on their website;
- Facilities are required to have a contingency plan for staffing shortages in the event of an outbreak or emergency;
- Facilities must implement a respiratory protection program compliant with OSHA that includes training and fit testing of all employees. Attestation of implementation of RPP is due by May 2021 but does not excuse the facility from meeting federal OSHA regulations.
The Phased Reopening attestation requires that facilities have a documented “Outbreak Plan,” that requires the following items related to communication:
- Methods to communicate information on mitigating actions implemented by the facility to prevent or reduce the risk of transmission, including if normal operations of the facility will be altered
- Methods to provide cumulative updates for residents, their representatives, and families of those residing in the facilities at least once weekly, in particular during a curtailed visitation period
- Written standards, policies and procedures that provide for virtual communication (e.g. phone, video-communication, Facetime, etc.) with residents, families, and resident representatives, in the event of visitation restrictions or an emergency
The outbreak plan must be posted on the facility’s website for public view no later than two (2) months from the enactment date of this Directive (i.e., October 10, 2020)
CMS-certified facilities are additionally required to have a documented communication plan to inform residents, their representatives, and families of the residents by 5 p.m. the next calendar day following the subsequent occurrence of either
- Each time a single confirmed infection of COVID-19 is identified, or
- Whenever three or more residents or staff with new-onset of respiratory symptoms occur within 72 hours of each other
All facilities must prominently display on their website and/or social media platforms and include in communications to families, guardians and the public, a phone number or method of communication for urgent calls or complaints.
All facilities are encouraged to follow CMS recommendations for communication when facilities cannot permit in-person visits as follows:
- Offer alternative means of communication for people who would otherwise visit, such as virtual communications (phone, video-communication, etc.);
- Create or increase email listserv communications to update families;
- Assign staff as primary contact to families for inbound calls, and conduct regular outbound calls to keep families up to date (e.g., a “virtual visitation coordinator”); offer a phone line with a voice recording updated at set times (e.g., daily) with the facility’s general operating status, such as when it is safe to resume visits;
- Host conference calls, webinars, or virtual “office hours” at set times, but at minimum on a weekly basis, when families can call in, or log on to a conference line, and facility staff can share the status of activities or happenings in the facility and family members can ask questions or make suggestions; and
- Update the facility’s website, at minimum on a weekly basis, to share the status of the facility and include information that helps families know what is happening in the loved one’s environment, such as food menus and any scheduled activities
The Phase 2 Indoor Visitation Attestation requires that facilities have a mechanism to collect informed consent from the residents and visitors, a location designated for indoor visitation, sufficient staff, a mechanism for appointments and sufficient PPE to permit visitation
Additional requirements for facilities to allow indoor visitation include:
- Screening and logging of all persons entering the facility and all staff at the beginning of each shift
- Actively screening all persons entering the building (except EMS personnel) for signs and symptoms of COVID-19 via temperature checks and completion of a questionnaire about symptoms and potential exposure. Persons with signs and symptoms and/or with potential exposure will be prohibited from entering the facility. Persons diagnosed with COVID-19 and who have not yet met criteria for the discontinuation of isolation will also be prohibited from entering.
- Establishing a designated area for visitors to be screened that accommodates social distancing and infection control standards
- Limiting visits to no more than two visitors at one time per resident. The facility must use appointments in order to limit the number of visitors inside the building at one time
- Requiring that permitted visitors follow precautions such as wearing a cloth face covering or face mask, following basic hand hygiene, practicing social distancing, etc.
- Requiring that facilities advise anyone entering the facility to monitor for signs and symptoms of COVID-19 for at least 14 days after exiting the facility
- Requiring informed consent from the visitor(s) and the resident in writing that they are aware of the possible dangers of exposure to COVID-19 for both the resident and the visitor and that they will follow the rules set by the facility in regard to visitation
A facility is considered to be in an “active outbreak” if either one of the below criteria is met:
- ≥1 facility-onset laboratory-confirmed COVID-19 case in a resident
- ≥2 laboratory-confirmed COVID-19 cases among health care professionals (staff) at the facility within a 14-day period
A facility is potentially considered to have “concluded” an outbreak when there are no symptomatic/asymptomatic probable or confirmed COVID-19 cases among employees or residents after 28 days have passed since the onset date or specimen collection date (whichever is later) of the last case at that facility.
The Local Health Department) will follow-up with facilities to confirm that no new (or probable) cases have occurred in the last 28 days. If there are any pending tests that were conducted during this 28-day period, testing will need to return negative before the outbreak can be considered concluded. Final determination of an outbreak’s conclusion is at the discretion of either NJDOH or local health officers
New COVID-19 positive cases reported in a long-term care facility after an officially “concluded” outbreak,” time would constitute the onset of a new outbreak.
No, A memorandum was issued on December, 9, 2020 titled “Respiratory Protection Program Attestation” and can be found here: https://nj.gov/health/legal/covid19/12-9-20_RPPMemo.pdf. This memorandum serves to clarify requirements in Executive Directive 20-0261 regarding the development and implementation of a Respiratory Protection Program (RPP).
ED 20-026 requires facilities to develop and implement a RPP that complies with the Occupational Safety and Health Administration (OSHA) respiratory protection standards for employees, and to submit an attestation of compliance to the Department by May 30, 2021. This requirement does not modify or otherwise affect facilities’ existing obligations under federal law to comply at all times with all applicable requirements of OSHA’s respiratory protection standards.
Visitations allowed by phase
The types of allowed visitation by phase are summarized in the table below:
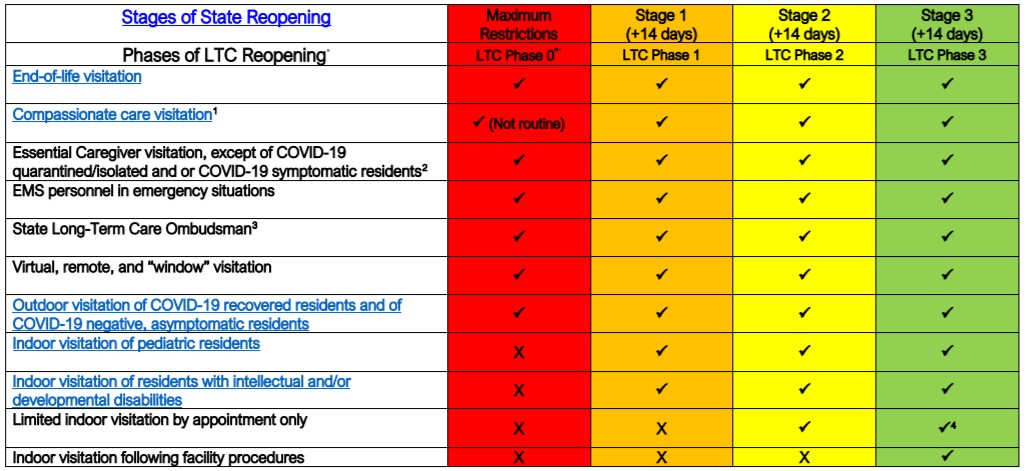
End-of-life visitations are allowed in every phase. Compassionate care visitations (which do not exclusively refer to “end-of-life situations”) are allowed in every phase but are not routine in Phase 0.
Essential caregiver visitations are allowed in every phase with the exception of those involving residents who are COVID-19 quarantined/isolated or COVID-19 symptomatic.
EMS personnel in emergency situations and the State Long-Term Care Ombudsman are allowed in every phase
Virtual, remote, and “window” visitations are allowed in every phase.
The types of visitation allowed vary by resident group and by phase.
Indoor visitation of pediatric residents is allowed in phases 1-3 (not allowed in phase 0).
Indoor visitation of residents with intellectual and/or developmental disabilities is allowed in phases 1-3 (not allowed in phase 0).
For visitations of residents who do not belong to the above two groups, limited indoor visitation by appointment only is allowed in phases 2-3 (not allowed in phases 0-1) if facility plans procedure are followed. Non-appointment visitation is only allowed in Phase 3.
Facilities should use the NJDOH COVID-19 Activity Level Index (CALI) Score here: https://www.nj.gov/health/cd/statistics/covid/index.shtml as additional information to determine how to facilitate indoor visitation. The CALI Score takes into account three factors for the region: (1) case rate (per 100,000) is calculated as a proportion of the population; (2) percent of COVID-like illness; and (3) the percent positivity. The CALI Score should be used to facilitate indoor visitation:
- CALI Score Low = Visitation should occur according to the core principles of COVID-19 infection prevention, NJDOH guidance and directives (beyond compassionate care, end-of-life and essential caregiver visits).
- CALI Score Medium = Consider limiting indoor visitation, although visitation may occur according to the core principles of COVID-19 infection prevention and NJDOH guidance and directives (beyond compassionate care, end-of-life and essential caregiver visits).
- CALI Score High or Very High = Visitation should only occur for compassionate care, end-of-life and essential caregiver situations according to the core principles of COVID-19 infection prevention, NJDOH guidance and directives. Facilities should check CALI scores on a weekly basis, every Thursday and are to cease all indoor visitation, except for compassionate care, end-of-life and essential caregiving if their region has entered into a High/Very High until the CALI score in the region returns to yellow/moderate or green/low for a minimum of two weeks.
Outdoor visitation of COVID-19 recovered residents and of COVID-19 negative, asymptomatic residents is allowed in every phase.
Activities and precautions by phase
Medically necessary trips (with face mask/covering) are allowed in every phase
Other type of trips (non-medically-necessary) are allowed in phases 2-3
Communal dining and other group activities among COVID-19 negative residents, asymptomatic residents and COVID-19 recovered residents is allowed in phases 1-3. Communal dining with additional limitations, precautions, and restrictions may be allowed in phase 1.
The following guidance applies to all phases.
Residents are to be tested weekly until all of the criteria below are true:
- No new facility-onset cases of COVID-19 are identified among residents and positive cases in staff (excludes residents with known COVID-19 infection on admission to facility)
- At least 14 days have elapsed since the most recent positive result
- During this 14-day period at least two weekly tests have been conducted with all individuals having tested negative
Residents who have been confirmed positive are to be retested whenever required according to CDS and CDC guidance.
Staff testing: Routine testing should be based on the extent of the virus in the community, therefore facilities should use the regional positivity rate reported in the COVID-19 Activity Level Index (CALI) Weekly Report: https://www.nj.gov/health/cd/statistics/covid/, in the prior week, as the trigger for staff testing frequency as follows:
|
Regional CALI Level |
Regional Percent Positivity Rate in the past week |
Minimum testing frequency |
|
Low |
<3% |
Once a Week* |
|
Moderate |
3-10% |
Once a Week* |
|
High/Very High |
>10% |
Twice a Week** |
Staff who have been confirmed positive are to be retested whenever required according to CDC and NJDOH guidance.
Any resident or staff who is newly symptomatic consistent with COVID-19 must be retested at the onset of symptoms, regardless of the interval between the most recent negative test and symptom onset.
During moderate and high CALI scores, facilities may request but not require, visitors to be tested on their own prior to coming to the facility (e.g., within 2–3 days) with proof of negative test results and date of test; the visitor can provide proof of a negative FDA approved or authorized point-of-care test collected and performed in the past 24 hours or PCR test collected and resulted no more than 3 days prior to the visit.
Facilities that have POC testing available are encouraged to use it as part of their visitor screening process, in particular during high/very high CALI scores in the region.
The following infection control precautions apply all phases:
- Enforcement of social distancing and other basic precautions (e.g., hand hygiene, wearing cloth face covering or face mask, restriction of movement indoors) for residents and visitors
- Ensuring that essential cleaning and disinfection supplies, PPE for staff, and an emergency stockpile of PPE are available
- Education of residents, staff, and visitors of basic precautions and hygiene (including how to use PPE for staff)
- Testing of residents and staff weekly
- Having at least 1 individual at each facility who is trained and assigned to on-site management of an Infection Prevention and Control (IPC) program and compliance
- Having a contract with an infection control service for the facility
- Having a respiratory protection program for staff, including medical evaluations, training, and fit testing
- Symptom screening for all persons before entry into a facility and for 14+ days after exiting a facility
- Symptom screening for staff at beginning of each shift and for residents during each shift (at minimum) and daily (at minimum)
- Limiting hours and number of visitors and requiring informed consent from visitors and residents
- Prohibiting visitation upon COVID-19 screening and/or if visitor has not discontinued isolation
- Prohibiting visitation by persons subject to 14-day quarantine travel advisory
- Reporting of key COVID-19 statistics (e.g., COVID-19 deaths and cases, resident beds and census, staffing shortages, PPE and hygiene supplies status, ventilator capacity and supplies) to National Healthcare Safety Network (NHSN) at least twice weekly
- Engage in resident cohorting to separate COVID-19 positive and negative residents
- Facilities shall implement universal eye protection, in addition to source control and other infection prevention and control measures, for all staff and for compassionate care or essential caregiver visitors unable to maintain social distancing when the NJDOH COVID-19 Activity Level Index (CALI) is Very High/High or Moderate (https://www.nj.gov/health/cd/statistics/covid/)
Entry of non-essential personnel is prohibited in phases 0-1, but is allowed in limited settings in phase 2. There is no such prohibition in phase 3.
Entry of volunteers is prohibited in phases 0-2 but is allowed in phase 3.